Reporting of Abdominal wall perforators prior to breast reconstruction
Technique: High flow CT Angiography (5 ml/s)
Cranial end - approx. 10 cm above the umbilicus
Caudal end - Pubic symphysis
Reconstruction: Ideal - 0.6 mm in axial
Can go with 1 mm also
Reporting:
Always discuss with the surgeon before finalizing the report. Preferably mapping in their company.
Conventional 3D will not be of help
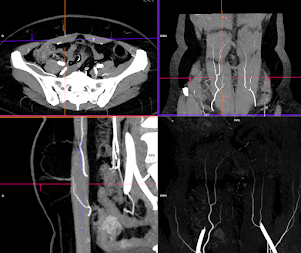
Load the sequence in 3D or if your PACS allows, load the angio sequence individually in axial/coronal and sagittal planes. Create thin MIP (15 to 30 mm) for each set of images.
Possible configurations in PACS or 3D workstation, as below with reference lines

Points to describe:
1. Describe the Deep Inferior epigastric artery and its branching
2. Identify the best perforator on each side, at it exit from the rectus muscle. Perforator's arising below umbilicus are preferred.
3. Give the following information & measurements:
a. Origin from the medial or lateral branch of the artery
b. Distance from the mid-line in transverse plane
c. Distance from the umbilicus in the coronal plane (you choose the one which is below the level of the umbilicus)
d. Diameter of the perforator at the exit, in the axial plane
e. The length of the intra-muscular course of the artery, that gives rise to the perforator, in the sagittal plane. Exclude, the course of artery, that is close to the surface.
Addendum:
1. Venous drainage of perforator
During the harvest of the flap, vein issues are the one of the common vascular complications. The drainage can be into both superficial and deep venous system and needs to be documented.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4115682/

Fig. 3: Venous drainage of abdominal wall perpetrators from DIEA
2. Perforators are better in patients who had pregnancy before
Prepared by Dr. Sharad Maheshwari
19.08.2022
updated: 01.04.2023
Based on request, i can do a live session on "how to report" on google meet / zoom
ReplyDelete